What is digital osteoarthritis?
It is the inevitable wear of cartilage with joint aging, as can be found in many other parts of the body (hip, knee, back...). Responsible for painful discomfort in hand use, it affects women more often than men.
Old joint fractures can lead to post-traumatic osteoarthritis, but it is most often "idiopathic", meaning without a clearly identified cause. Sometimes a familial predisposition can be identified.
We distinguish thumb arthritis (osteoarthritis of the thumb base) which poses quite specific problems, and digital osteoarthritis whose term usually corresponds to involvement of the other fingers.
How does digital osteoarthritis present?
The 3 main signs are pain, deformations and joint stiffness.
The joint wears out over many years, and symptoms are generally progressively increasing in intensity. At the beginning, joint pain appears from cartilage loss and direct bone-to-bone contact.
Joint inflammation leads to progressive distension of ligaments and growth of peripheral bone outgrowths (osteophytes), both leading to visible deformation.
The joint progressively destroys itself and loses mobility, pain causing loss of strength through muscle deconditioning. This evolution of osteoarthritis can be slow and progressive, or accompanied by transient inflammatory flares with joint swelling and severe pain.
A simple X-ray allows diagnosis of the disease and its evolutionary stage.
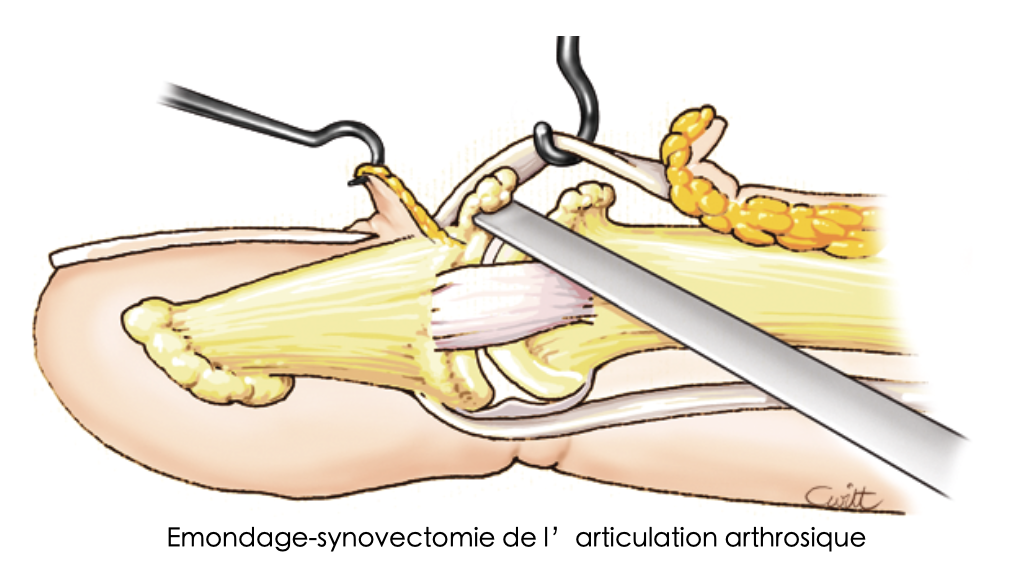
Debridement-synovectomy of the arthritic joint
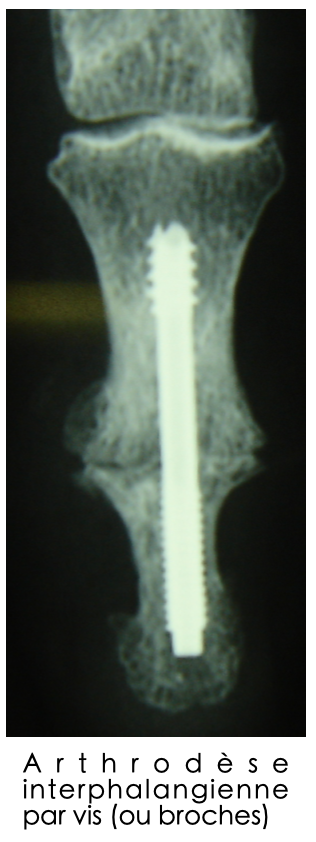
Interphalangeal arthrodesis with screw (or pins)
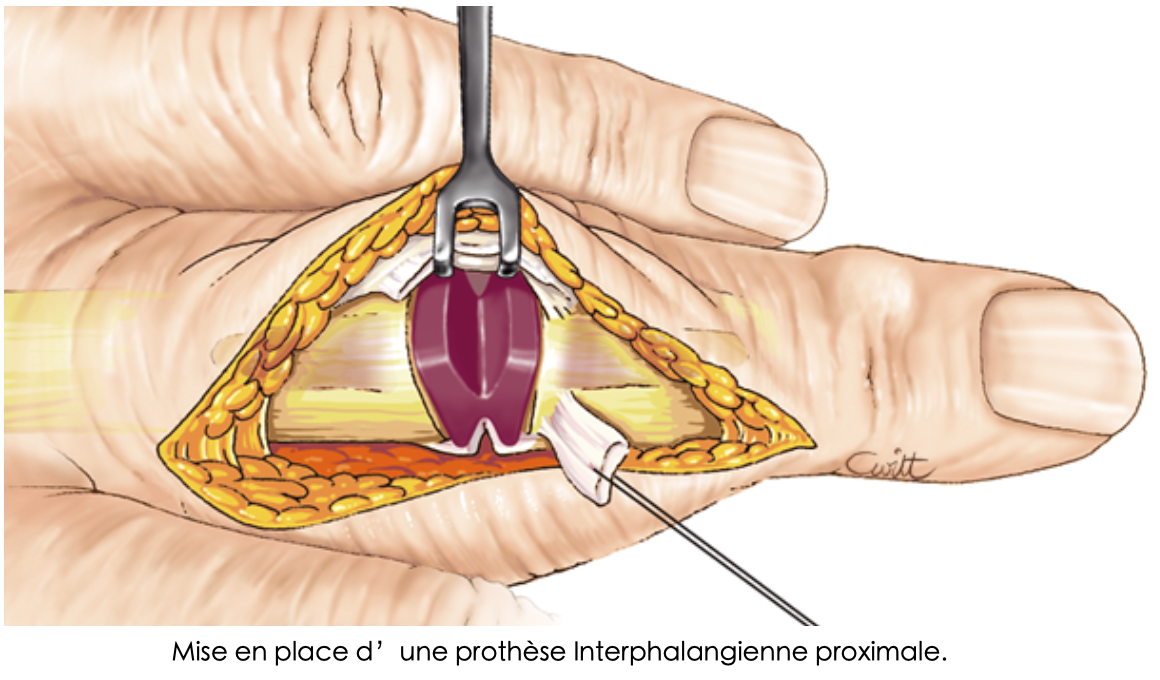
Placement of a proximal interphalangeal prosthesis
I have digital osteoarthritis, what can be done?
There is no truly scientifically validated preventive treatment. There is also no absolute relationship between the extent of radiographic joint destruction and symptom intensity.
Some minimally destroyed joints cause significant pain, and conversely, major radiographic osteoarthritis is relatively well tolerated. It is therefore not necessary to be alarmed, and treatment may not be mandatory.
Medical treatment
When pain and discomfort increase, treatment with splints and analgesics is initially proposed.
Anti-inflammatory drugs can help get through a painful flare, but treatment that is too strong or too long should be avoided.
Surgical treatment
If medical treatment is no longer sufficient, surgery can be discussed. The type of intervention depends on the joint involved and the extent of functional impairment.
- Surgical joint cleaning (synovectomy): can be performed when mobility is well preserved
- Prosthesis: preserving mobility, feasible on the proximal interphalangeal joint (in the middle part of the finger)
- Arthrodesis: definitive blocking by bone fusion, preferable for the distal interphalangeal joint (just before the nail) due to its small size
Your doctor and surgeon are your best advisors when choosing treatment.
I'm going to have digital osteoarthritis surgery... what will happen to me?
The procedure is performed under regional anesthesia. Depending on the surgical procedure performed and the number of joints treated simultaneously, hospitalization can be either outpatient or for a few days (2-3 days).
Early finger mobilization is then encouraged with sometimes a few physiotherapy sessions. Skin healing requires 15 days to 3 weeks of dressings and caution, with the hand often quickly usable for light activities.
Effectiveness on pain is generally very satisfactory, improving hand function. Increased mobility, strength and treatment of deformations is much rarer.
Is digital osteoarthritis surgery risk-free?
No, of course not. Although it is a codified, routine and mastered procedure, the risk exists, as with any surgery, even if complications are rare.
We mainly find, even if all precautions are taken:
- Healing difficulties
- Hematoma
- Local infection
- Algodystrophy
- Anesthetic complications
- Failure of bone consolidation in arthrodesis
- Scar hypersensitivity
- Prosthesis wear
- Finger deviation
- Stiffness and residual impairment
What is the risk of not having surgery?
There is no serious risk in not treating osteoarthritis. However, as osteoarthritis continues its work, pain, deformations and discomfort increase, as much as hand function deteriorates.
Need a consultation?
Our specialists assess your situation and propose appropriate treatment.
Make an appointment