What is ulnar nerve compression syndrome?
It is the compression of the ulnar nerve during its passage on the posterior side of the elbow, or more rarely at the wrist. The ulnar nerve is one of the 3 nerves of the hand. Its role is sensation, motor function of the last 2 fingers of the hand and grip strength.
At the elbow passage, it travels in the epitrochleo-olecranon groove (in contact with the joint) under a fibrous arcade of the flexor carpi ulnaris (FCU). This canal is the most frequent compression site.
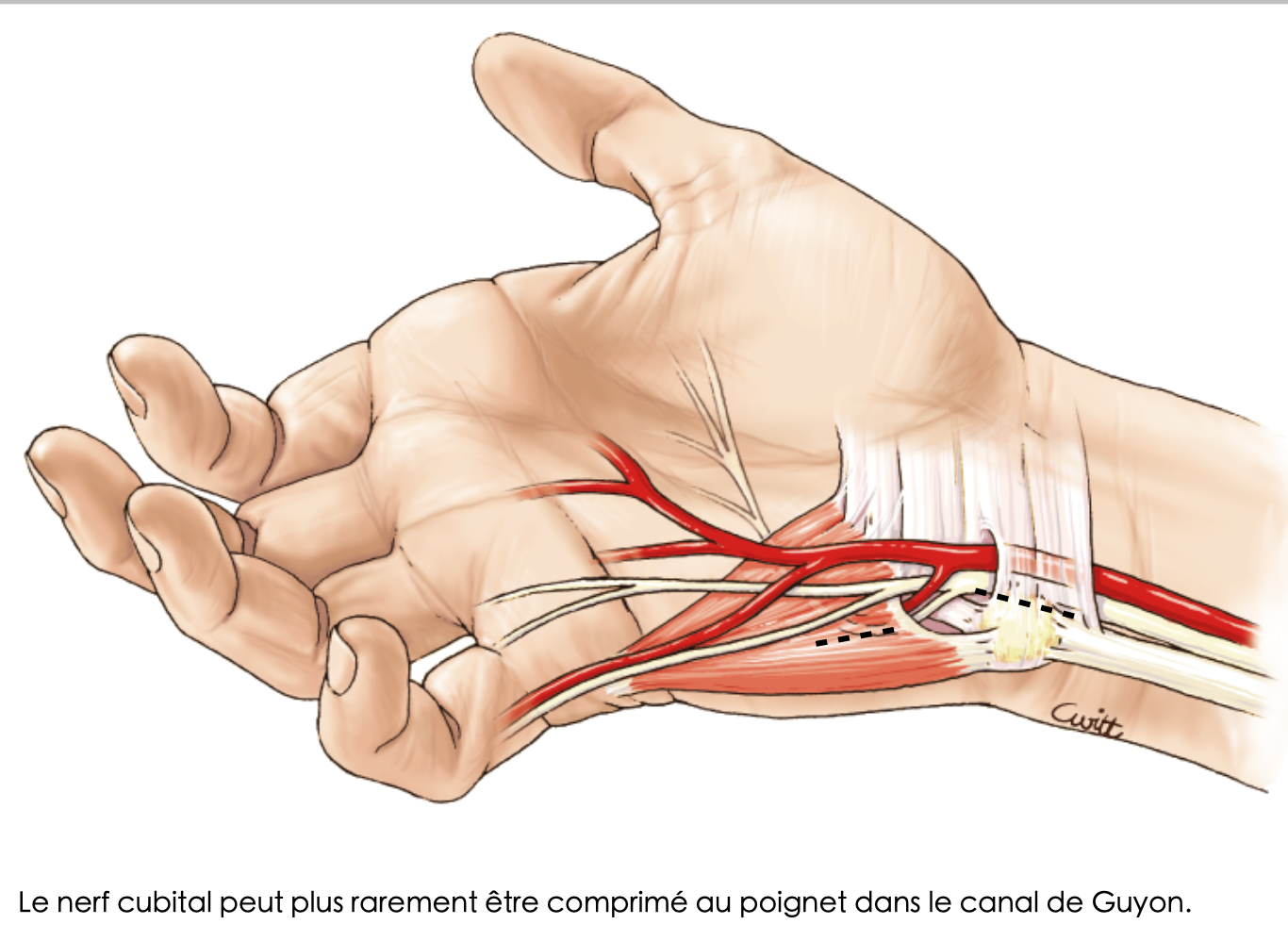
More rarely it can be compressed at its passage through the wrist in Guyon's canal (its compression is then similar to carpal tunnel syndrome) and more difficult to diagnose.
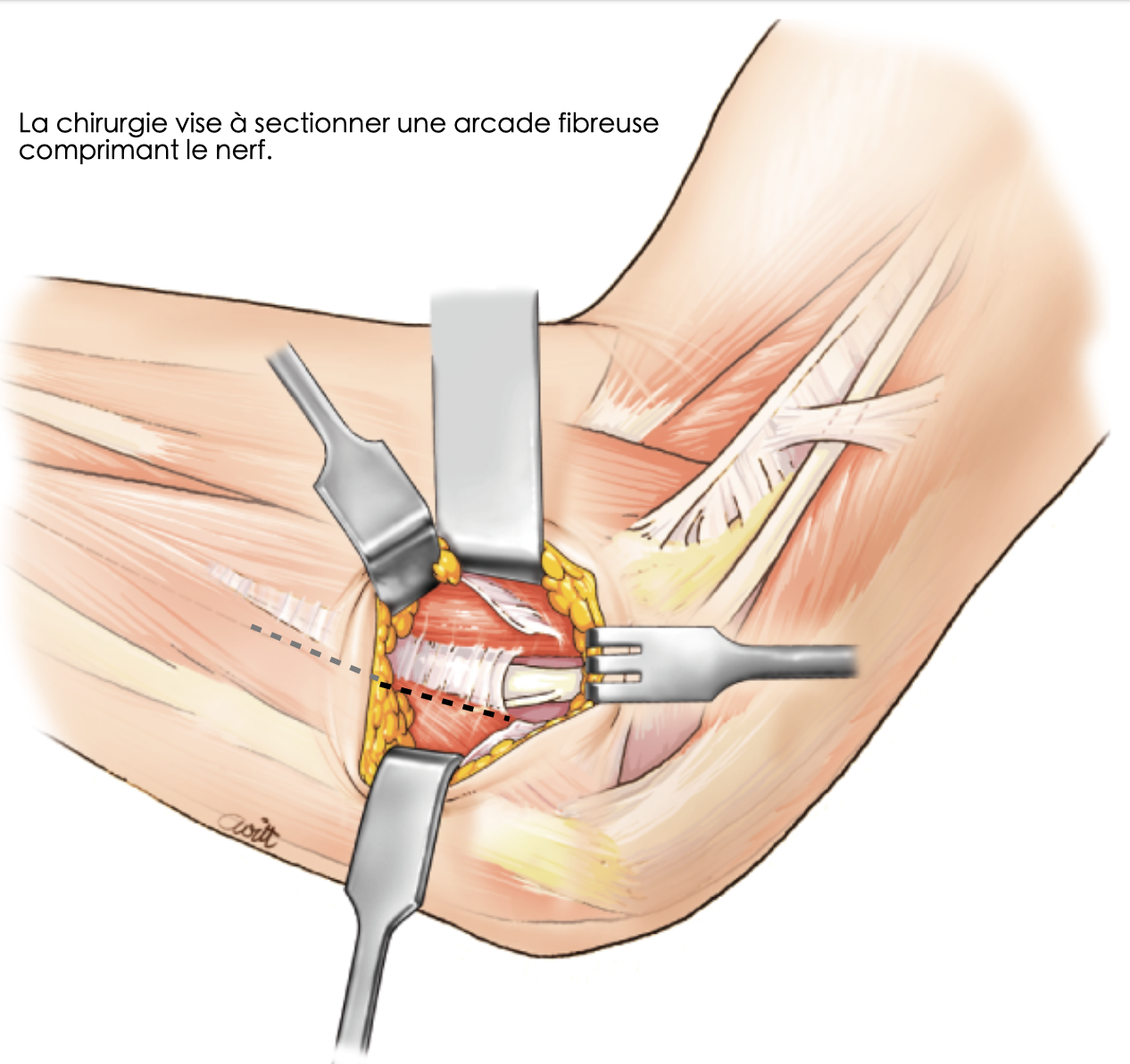
Surgery aims to section a fibrous arcade compressing the nerve
The ulnar nerve can more rarely be compressed at the wrist in Guyon's canal
How does this ulnar nerve compression manifest?
In most cases, the symptoms are those related to nerve compression. We find paresthesias ("pins and needles") in the last 2 fingers.
At the beginning
Paresthesias are mainly nocturnal, possibly related to elbow flexion position.
When the disease progresses
Paresthesias appear during the day, associated with decreased sensations (hypoesthesia).
Severe involvement
Loss of strength, endurance, with appearance of cramps and hand muscle wasting occur, indicating progressive nerve destruction.
This is the most classic presentation, but the disease presentation is sometimes more insidious or incomplete.
Diagnosis
An electromyogram (EMG) must be performed by a specialist (neurologist or rheumatologist most often): it measures nerve conduction velocity and looks for slowing at the elbow or wrist passage.
This examination confirms the existence of the disease, looks for other associated compression sites and specifies the state of the nerve.
My ulnar nerve is compressed, what can be done?
Several parameters come into play for the treatment decision, such as age, extent of discomfort, EMG results, professional activity, speed of progression... all these parameters are best evaluated by your doctor and surgeon during consultation.
Often the existence of bothersome symptoms and EMG confirmation motivate surgical decompression treatment, because the ulnar nerve is a susceptible nerve, whose recovery is slow and difficult when nerve destruction has begun. It is preferable to release it before the appearance of significant damage.
I'm going to have ulnar nerve decompression surgery... what will happen to me?
Surgical principle
Surgery aims to section the fibrous arcade of the FCU to increase canal volume and thus decompress the nerve.
- At the wrist: the operation is similar by sectioning all anatomical structures responsible for compression
- At the elbow: sectioning the fibrous arcade can sometimes cause nerve dislocation in elbow flexion: the surgeon then proceeds to move the nerve in front of the elbow to limit this instability, performing an anterior transposition of the nerve
Procedure
Ulnar nerve release (or transposition) is a routine, short procedure, most often performed under regional anesthesia, on an outpatient basis. Two weeks of healing are necessary, with a small dressing.
Recovery
Symptoms are often only slightly modified immediately after surgery, the nerve often taking several weeks or even more than 6 to 9 months to recover from compression.
When nerve damage is severe, nerve regrowth occurs (depending among other things on age, smoking...), long and sometimes incomplete. In this last case we can sometimes witness a "false worsening" of post-operative symptoms, the time for the nerve to regrow to the hand in the following months and for recovery to finally begin.
Is ulnar nerve surgery risk-free?
No, of course not. Although it is a codified, routine and mastered procedure, the risk exists, as with any surgery, even if complications are rare.
We mainly find, even if all precautions are taken:
- Healing difficulties
- Hematoma
- Local infection
- Incomplete nerve release
- Algodystrophy
- Anesthetic complications
- Section of a nerve branch
- Reinnervation pain (exuberant nerve regrowth after release in severe forms)
- Nerve instability dislocating in elbow flexion
What is the risk of not having surgery?
The risk is the continuation of the disease leading to complete or almost complete nerve destruction: permanent finger anesthesia, loss of strength and hand deformation, leading to major impairment.
Moreover, the destroyed nerve can cause neuropathic pain particularly difficult to control.
At this stage surgical treatment can still be proposed, but the final result is very often incomplete and disappointing, leaving permanent disability.