What are epicondylalgias?
They include tendinitis around the elbow with epitrochleitis (medial side) and epicondylitis (lateral side). The latter is the most common.
Like many tendinitis, this disease is often the consequence of a recent increase in hand solicitation (gardening, DIY, repetitive professional or domestic maneuvers, change of workstation...) or poor posture during unusual movements (sport, bodybuilding, musical instrument...).
Tendon aging with age can favor the appearance of these tendinitis. Sometimes a specific triggering factor can be found (sudden movement, direct impact, or suddenly interrupted movement,...). Prolonged repetition of the same professional or domestic gestures can lead to epicondylitis through microtraumatic "wear".
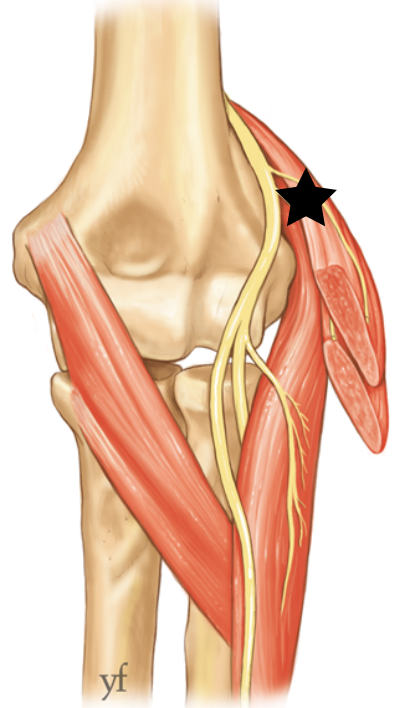
It is more appropriate to speak of epicondylalgia, as it is more likely a tendon degeneration, and local inflammation can lead to compression of a nerve branch (radial nerve) passing in contact with the affected tendons.
How do epicondylalgias most often present?
Pain localized at the lateral edge of the elbow appears, especially during forceful maneuvers. Traction on tendons and palpation of painful areas during clinical examination associated with trauma or gestural context allow diagnosis.
Imaging examinations
An imaging examination is sometimes requested by your doctor or surgeon when the clinical picture requires it, but diagnosis is in the vast majority of cases only clinical.
Ultrasound and MRI can find a tendon tear, which only indicates the age of the epicondylitis and tendon degeneration, but is not a sign of any emergency.
Radial nerve release and tendon lengthening
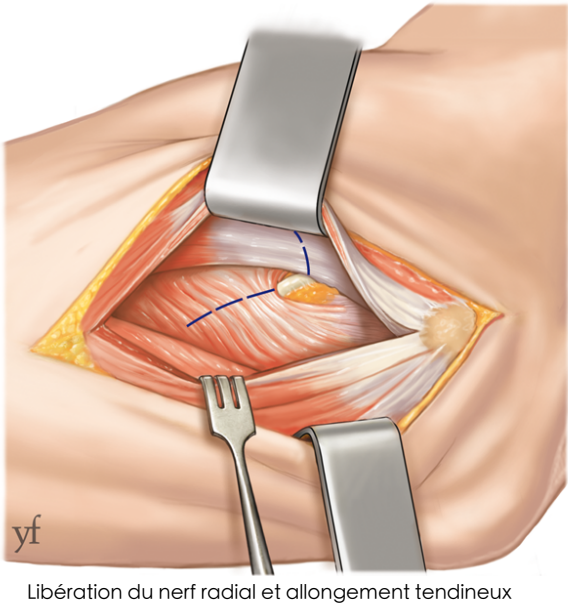
Surgical technique of tendon lengthening
I have epicondylitis, what can be done?
At the beginning the condition is acute and can sometimes be quickly corrected if the causal activity is stopped. When the disease sets in, it becomes chronic and its treatment is longer and more difficult.
Conservative treatment
- Rest splint placed at night to relax tendons
- Physiotherapy sessions and diligent self-rehabilitation with stretching, deep massage and eccentric strengthening (basis of conservative treatment)
- Corticosteroid infiltration (can accelerate recovery, but does not always have complete and permanent effectiveness, exposing to sometimes significant recurrence of pain if gestures are not modified, as it only masks symptoms)
⚠️ Modification of gestures - ESSENTIAL
Modification of the gestures responsible for tendinitis is ESSENTIAL to hope for healing, and especially the absence of disease recurrence.
This involves limiting painful activities for the time necessary for complete recovery, then supervision by a professional when resuming the causal activity (sport, music, workstation...) to correct poor postures.
Surgical treatment
When the disease resists this medical treatment, or has been present for long months, surgery is required.
It consists of lengthening the responsible tendons to reduce traction on their painful insertions. When the radial nerve is compressed, its release is performed at the same time.
I'm going to have epicondylitis surgery... what will happen to me?
It is a routine, short procedure, most often performed under regional anesthesia, on an outpatient basis.
Surgical principle
Surgery aims to lengthen the responsible tendons to reduce tension on them, and release the radial nerve if symptoms suggest this associated compression.
Healing
Two weeks of healing are necessary, with a small dressing. For 1 month, it is not recommended to carry loads, under penalty of risk of tendinitis recurrence. A splint is sometimes recommended to rest the wrist after the intervention.
Recovery
Pain disappearance is very variable in speed and intensity, with the existence of an old chronic condition potentially slowing healing.
It is more often an improvement in pain and therefore discomfort, rather than complete healing.
Obviously, modification of the gestures responsible for tendinitis is ESSENTIAL to hope for healing, and especially the absence of disease recurrence.
Is epicondylitis surgery risk-free?
No, of course not. Although it is a codified, routine and mastered procedure, the risk exists, as with any surgery, even if complications are rare.
We mainly find, even if all precautions are taken:
- Healing difficulties
- Hematoma
- Local infection
- Algodystrophy
- Anesthetic complications
- Occurrence of transient radial nerve irritation
- Scar hypersensitivity
There is also the risk that surgical treatment does not lead to pain relief because the disease is the consequence of many factors.
What is the risk of not having surgery?
The risk is the continuation of the disease and pain with increasing discomfort for increasingly light activities.
Chronification of tendinitis makes recovery more difficult and more often incomplete.
Persistent elbow pain?
Consult our specialists for accurate diagnosis and appropriate treatment.
Make an appointment